Our heart is the most fascinating organ of the body. It is the only part that is constantly moving, pumping 5 to 6 liters of blood to all other organs. If it stops even for 3 minutes, we will die without any chance of revival. The heart’s function relies on several intricate mechanisms that ensure its efficient operation.
Natural Electrical Conduction System of heart
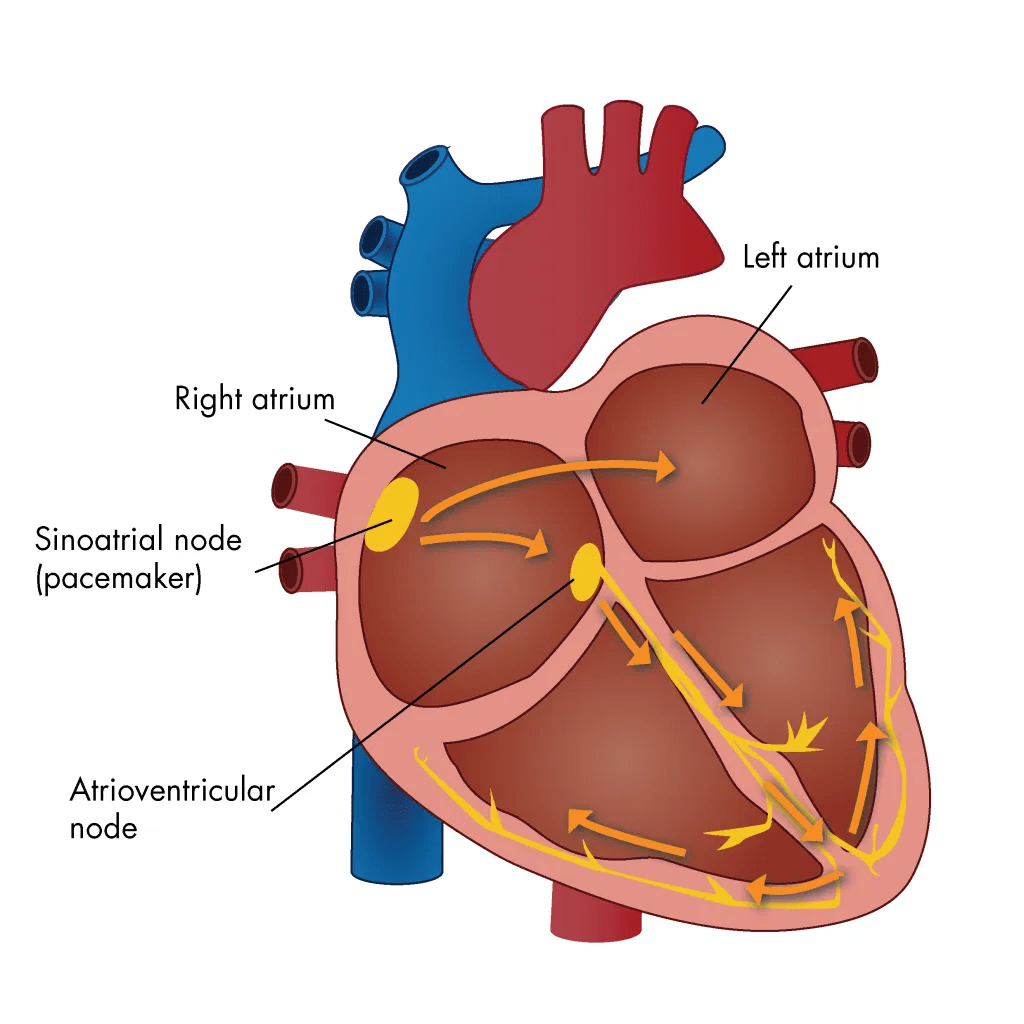
The heart’s conduction system is one of the essential examples of our body’s complex structure. It is made up of specialized “wires” which are modified muscle fibers. The heart’s electrical activity starts in the right upper chamber in the part called the sinus node, which is known as the natural pacemaker of the heart. From here, the electrical signal travels almost instantaneously to the left upper chamber, allowing both upper chambers to contract simultaneously. Following this, the electrical signal travels downwards through the atrioventricular (AV) bundle to the AV node, where there is a brief delay. After this delay, the signal spreads to both lower chambers, again causing them to contract almost simultaneously, but only after the upper chambers have done so. This sequential contraction is crucial for the proper functioning of the heart and the adequate transit of blood throughout the body. Any disruptions in this finely-tuned system can lead to serious complications, which we will discuss subsequently.
Slow Heart Rate (Bradyarrhythmias)
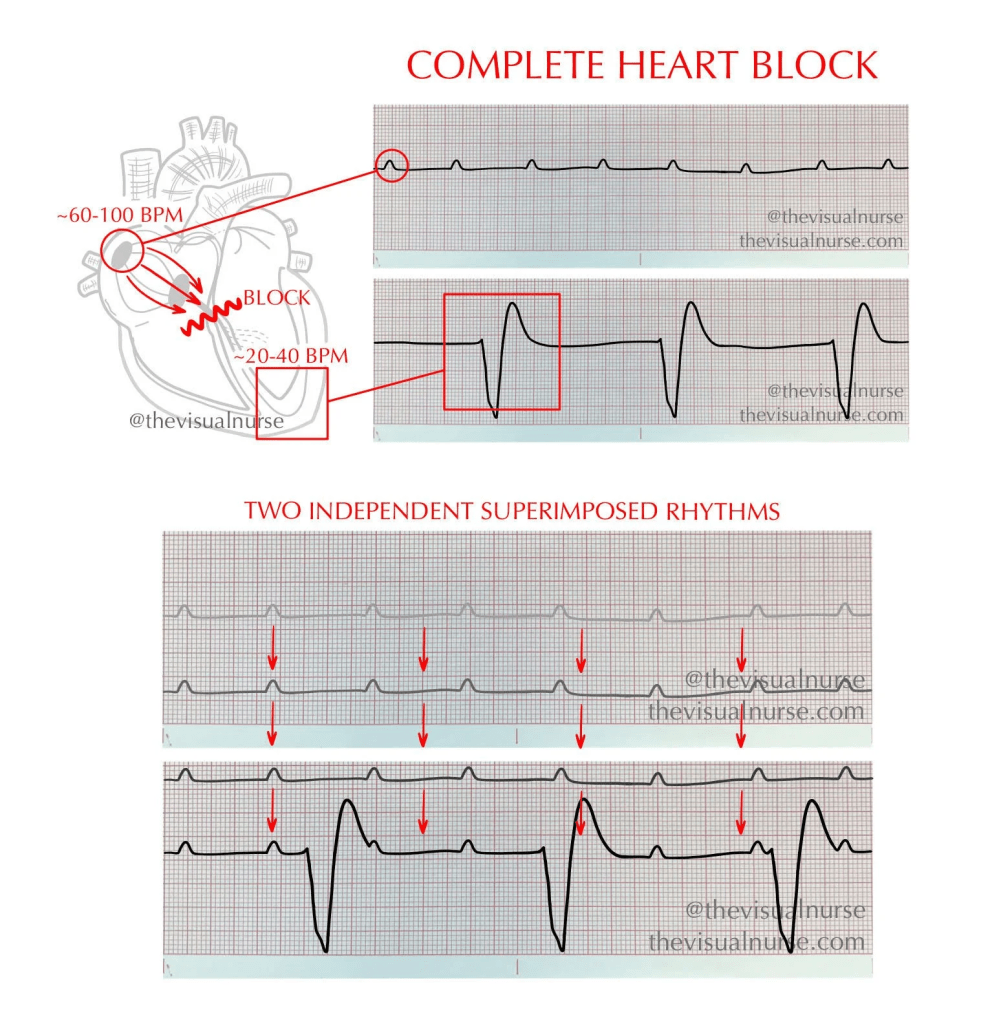
The first kind of arrhythmias encompasses those where the heart rate becomes significantly slow, a condition that can be life-threatening. Patient can have easy fatiguability, frequent fainting episodes or shortness of breath. The causes of this can be varied. Often, they arise when the sinus node becomes diseased, leading to a delayed generation of the electrical signal. Alternatively, the electrical wires may become damaged, causing the electrical signals to travel very slowly or not at all. These issues can frequently occur due to heart rate-lowering medications or electrolyte imbalances, such as elevated potassium levels in the blood. Stopping the drug or correcting the electrolyte imbalance can sometimes restore the normal heart rhythm and rate. However, in many cases, there may be permanent damage caused by age or diseases like fibrosis, which complicate recovery. In emergency conditions where the heart rate drops suddenly and becomes life-threatening, a temporary pacemaker may be required to stabilize the patient and potentially save their life.
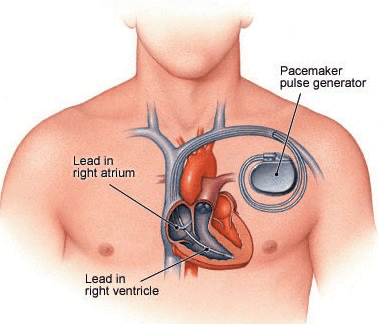
In scenarios where normal rhythm cannot be restored despite above mentioned interventions, specialized devices that provide artificial electrical signals may need to be implanted. These devices, known as permanent pacemakers, consist of wires that are fixed within the right-sided heart chambers. A battery, known as the pace generator, is typically placed beneath the right or left clavicle by creating a small pocket beneath the skin. Depending on whether only the lower chambers are wired or both the upper and lower chambers are wired, pacemakers can be classified as single-chamber or double-chamber devices. Over time, these pacemakers have become increasingly sophisticated, enabling them to perform a variety of functions to maintain a near-natural heart rhythm.
Fast Heart Rate Problems ( Tachyarrythmias)
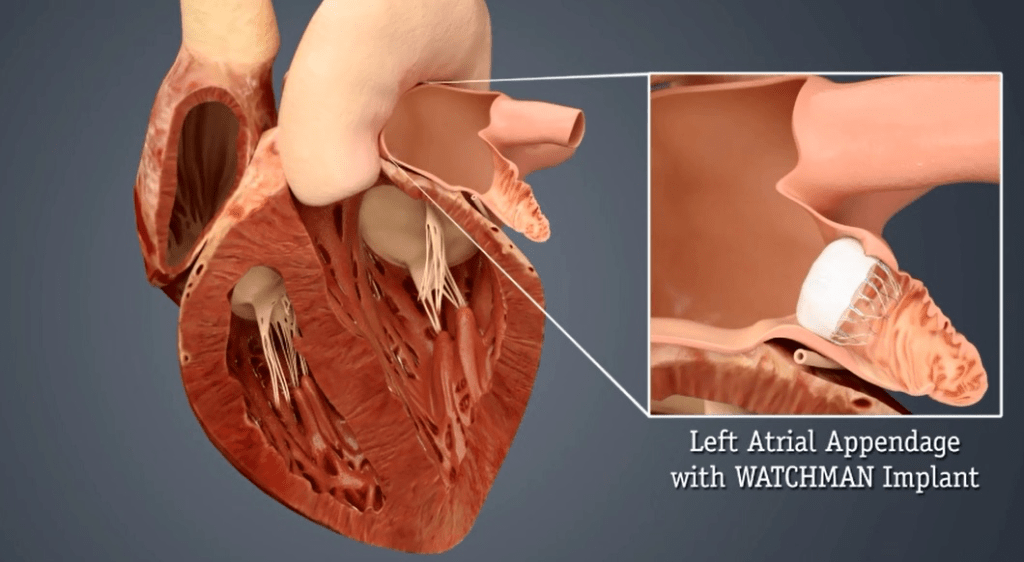
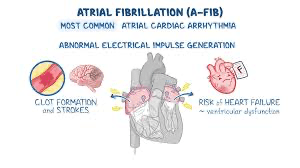
Another type of arrhythmia, categorized as tachyarrhythmias, is more complex and occurs when the heart rate becomes excessively high. These arrhythmias can present in several forms, with atrial fibrillation (AF) being the most prevalent arrhythmia. In AF, the atria contract very quickly and irregularly, which, in turn, causes the ventricles to also contract rapidly and without rhythm. This can result in two significant problems: first, heart failure, where the heart is unable to pump enough blood to vital organs; second, ineffective atrial contractions may lead to blood stagnation and clot formation. These clots can dislodge and travel to various organs, potentially resulting in life-threatening cardio-embolic events, most notably brain strokes . The treatment of atrial fibrillation addresses two main aspects: the use of blood-thinning medications to reduce clot risk, and medications aimed at controlling heart rhythm and rate. For patients where blood-thinner medications are contraindicated, left atrial appendage closure devices can be implanted to reduce the risk of stroke. If symptoms remain persistent despite these interventions, further investigations including electrophysiological studies followed by ablation may be indicated to correct the underlying problem.
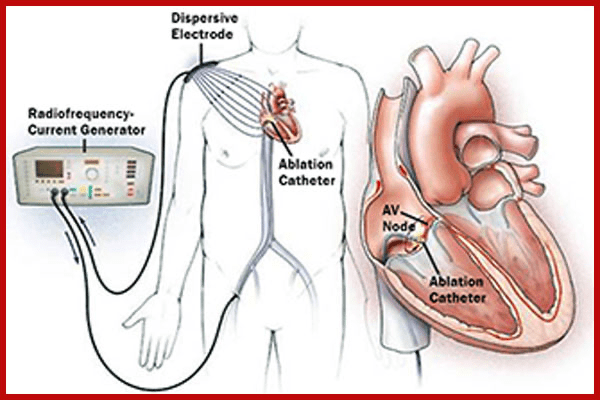
A second important type of arrhythmia is supraventricular tachycardia (SVT), which is usually benign but can occasionally cause significant symptoms that may even become life-threatening. The underlying cause of these arrhythmias typically involves an extra “wire” in the conduction system, which triggers rapid and repetitive activation of the heart. Many patients with SVT can stabilize their condition with medications, while others may require an electrophysiological study (EPS) combined with radiofrequency ablation (RFA) or other types of ablation. This approach identifies and eliminates the extra conduction pathways, often successfully curing the condition.
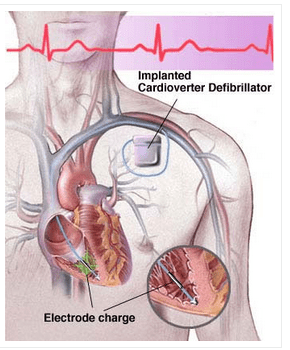
The most dreaded forms of arrhythmias are ventricular tachycardia and ventricular fibrillation, both of which are life-threatening if not managed immediately. These situations can arise from a heart attack or can complicate conditions such as cardiomyopathy. Some individuals have a genetic predisposition to develop these severe arrhythmias, making immediate recognition and intervention essential. For emergency management of unstable patients experiencing these arrhythmias, delivering an electrical shock using an external defibrillator is essential. In cases where the patient is stable, various antiarrhythmic drugs may be employed to suppress the arrhythmias. However, if the patient is unstable, electrical cardioversion or defibrillation remains the treatment of choice to restore a normal rhythm effectively. For long-term management, an automated implantable cardioverter-defibrillator (AICD) may be warranted in patients at high risk. This device automatically detects the rhythm issue and either activates fast pacing or gives a measured low intensity shock to restore the normal rhythm. Additionally, some patients may require further electrophysiological studies and ablation to address the causative pathways of these dangerous arrhythmias.
In conclusion our heart is truly a marvel, working tirelessly every second of our lives. Sometimes, however, its natural rhythm can go wrong—either too slow, too fast, or irregular. While this may sound frightening, the good news is that medical science today offers many effective solutions. From simple medicines to advanced devices like pacemakers and defibrillators, doctors can restore the heart’s rhythm and protect patients from dangerous complications such as heart failure or stroke. The most important step is awareness: do not ignore warning signs like unexplained fatigue, palpitations, dizziness, or fainting spells. Early consultation with a heart specialist can make all the difference, ensuring timely treatment and a longer, healthier life.
Dr. Tamiruddin A. Danwade.
Dr. Tamiruddin A. Danwade is a highly qualified medical professional holding the following degrees: MD in Medicine, DNB in Cardiology, and is a Fellow of the Society for Cardiovascular Angiography and Interventions (FSCAI) in the USA. He specializes in interventional cardiology, a field dedicated to the diagnosis and treatment of heart conditions through minimally invasive procedures.
हृदयाचे अनियमित ठोके (कार्डियाक अरिदमिया)
आपले हृदय हे शरीरातील सर्वात विलक्षण अवयव आहे. हा शरीरातील एकमेव भाग आहे जो सतत चालू असतो आणि दर मिनिटाला ५ ते ६ लिटर रक्त शरीरातील इतर अवयवांपर्यंत पोहोचवतो . जर ह्रदय ३ मिनिटे जरी थांबले, तर आपण पुन्हा जिवंत होऊ शकत नाही. हृदयाचे कार्य अनेक गुंतागुंतीच्या यंत्रणांवर अवलंबून आहे ज्यामुळे ते सुरळीत चालते.
⸻
हृदयातील नैसर्गिक विद्युत वहन प्रणाली
हृदयातील ही वहन प्रणाली ही शरीराच्या गुंतागुंतीच्या रचनेचे उत्कृष्ट उदाहरण आहे. ही प्रणाली विशेष “वायर्स” म्हणजेच बदललेले स्नायूंचे तंतू यांच्यापासून तयार झालेली असते. विद्युत सिग्नल हृदयाच्या उजव्या वरच्या कप्प्यात असलेल्या सायनस नोड पासून सुरू होतो, ज्याला हृदयाचा नैसर्गिक पेसमेकर म्हटले जाते. इथून हा सिग्नल डाव्या वरच्या कप्प्यात जातो आणि दोन्ही वरचे कप्पे एकाच वेळी आकुंचन पावतात. त्यानंतर सिग्नल खालच्या कप्प्यांकडे जातो, पण त्याआधी एव्ही (AV) नोडमध्ये थोडा विलंब होतो. या विलंबामुळे वरचे कप्पे आधी आकुंचन होतात आणि मग खालचे कप्पे. ही साखळी पद्धती हृदयाच्या कार्यासाठी आणि रक्तप्रवाहासाठी अत्यंत महत्त्वाची असते. या प्रणालीत बिघाड झाला तर गंभीर समस्या निर्माण होऊ शकतात.
⸻
मंद ठोके (ब्रॅडिअरिदमिया)
जेव्हा हृदयाचे ठोके खूपच मंद होतात, त्याला ब्रॅडिअरिदमिया म्हणतात. यात थकवा, श्वास लागणे, वारंवार बेशुद्ध पडणे अशी लक्षणे दिसू शकतात. हे अनेक कारणांनी होऊ शकते—सायनस नोड चा आजार , विद्युत वहन करणारे तंतू खराब होणे, औषधांचा परिणाम किंवा रक्तातील पोटॅशियमचे जास्त प्रमाण. बहुतेकदा औषध थांबवल्यावर किंवा इलेक्ट्रोलाइट्स नीट केल्यावर लय सुधारते. पण बऱ्याच वेळा वय वाढल्यावर होणारे बदल किंवा आजारामुळे कायमस्वरूपी नुकसान झाल्याने पेसमेकरची गरज भासू शकते.
पेसमेकर हे लहान यंत्र असून त्यामध्ये बॅटरी (पेस जनरेटर) आणि तारा असतात, ज्या हृदयाच्या उजव्या कप्प्यात बसवल्या जातात. हे यंत्र कृत्रिम विद्युत सिग्नल देऊन हृदयाची गती नियंत्रित करते. आजकालचे पेसमेकर अधिक प्रगत असून जवळपास नैसर्गिक गती राखू शकतात.
⸻
जलद ठोके (टॅकीअरिदमिया)
जेव्हा हृदयाची गती खूपच जास्त होते, त्याला टॅकीअरिदमिया म्हणतात. यात विविध प्रकार आहेत.
एट्रियल फिब्रिलेशन (AF):
हा सर्वाधिक आढळणारा अरिदमिया आहे. यात वरचे कप्पे वेगाने आणि अनियमितपणे आकुंचन पावतात, ज्यामुळे खालचे कप्पेही अनियमित ठोके देतात. यात दोन मोठे धोके असतात—
1. हृदय शरीराच्या गरज इतके रक्त पंप करू न शकने (Heart Failure)
2. ह्रदयात रक्त साचून गाठी तयार होणे आणि शरीरातात इतरत्र पसरणे मुख्यतः मेंदूच्या रक्तवाहीन्यात जावून स्ट्रोक होणे.
उपचारामध्ये रक्त पातळ करणारी औषधे, हृदयाची गती व लय नियंत्रित करणारी औषधे वापरली जातात. काही रुग्णांमध्ये रक्त-पातळ करणारी औषधे न देता डाव्या एट्रियल अपेंडेजमध्ये closure device बसवले जाते. औषधोपचार अपुरे ठरल्यास इलेक्ट्रोफिजिओलॉजिकल तपासण्या व एब्लेशनद्वारे समस्या दुरुस्त करता येते.
• सुप्राव्हेंट्रिक्युलर टॅकीकार्डिया (SVT):
हा प्रकार सामान्यतः सौम्य असतो, पण कधीकधी गंभीर लक्षणे देऊ शकतो. यात हृदयाच्या विद्युत वहन प्रणालीत एक जादा “वायर” असल्यामुळे ठोके जलद होतात. औषधोपचाराने नियंत्रण शक्य असते; परंतु काही रुग्णांमध्ये EPS व रेडिओफ्रिक्वेन्सी एब्लेशन करून हा जादा वायर कायमस्वरूपी नष्ट केली जाते.
• व्हेंट्रिक्युलर टॅकीकार्डिया व व्हेंट्रिक्युलर फिब्रिलेशन:
हा अत्यंत धोकादायक प्रकार असून त्वरित उपचार न मिळाल्यास मृत्यू होऊ शकतो. हे अनियमित ठोके हृदयविकाराच्या झटक्यानंतर किंवा हृदयाच्या स्नायूंच्या आजारात ( cardiomyopathy) होऊ शकतात. आपत्कालीन परिस्थितीत बाह्य डिफिब्रिलेटरद्वारे विद्युत धक्का ( External Electric Cardioversion) देऊन रुग्णाचे प्राण वाचवता येतात. दीर्घकालीन व्यवस्थापनासाठी काही रुग्णांना AICD (ऑटोमॅटिक इम्प्लांटेबल कार्डिओव्हर्टर-डिफिब्रिलेटर) लावला जातो. हे यंत्र धोकादायक ठोके आपोआप ओळखते आणि विद्युत धक्का ( small electric shock) देऊन लय सुधारते.
⸻
निष्कर्ष
आपले हृदय खरोखरच अद्भुत आहे. पण कधी कधी त्याची लय विस्कळीत होते—कधी खूप मंद, कधी खूप जलद, तर कधी अनियमित. हे ऐकायला भितीदायक वाटते, पण आजच्या वैद्यकशास्त्रात औषधोपचारापासून पेसमेकर व डिफिब्रिलेटर यंत्रापर्यंत अनेक प्रभावी उपाय उपलब्ध आहेत. सर्वात महत्त्वाचे म्हणजे जागरूकता—अकारण थकवा, धडधड, चक्कर येणे किंवा बेशुद्ध होणे याकडे दुर्लक्ष करू नका. योग्य वेळी हृदयरोगतज्ज्ञांचा सल्ला घेतल्यास योग्य उपचार मिळतात आणि आयुष्य निरोगी व दीर्घ होऊ शकते.
डॉ. तमिरुद्दीन ए. दानवाडे
ह्रदयरोग तज्ञ
नवी मुंबई.

Leave a comment