Our heart is a natural pump with tremendous efficiency. It supplies blood to the whole body. Coronary arteries are small but vital blood vessels that supply blood to the heart itself. Blockades in these blood vessels mainly due to cholesterol deposition lead to minor or major heart attacks which are potentially life threatening.
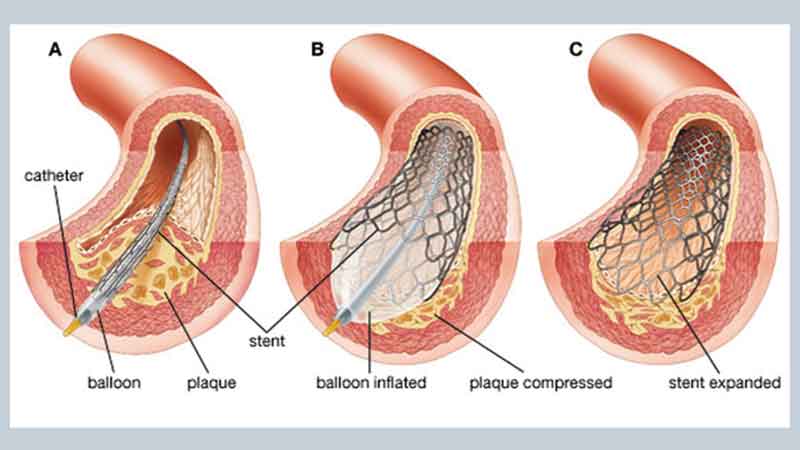
Historically bypass surgery was the only treatment option available for these blockades. This is a supra-major surgery with its own drawbacks like long recovery time, perioperative morbidity and mortality. In 1977, Dr Andreas R. Grüntzig invented the less invasive treatment option – Coronary Angioplasty. Angioplasty is a percutaneous procedure where the cardiologists pass a balloon over a wire in the coronary arteries through a small tube-like guiding catheter, and blockades are dilated to improve the blood flow through them. Initially, it was a crude method, nothing else was feasible, subsequently, stents were invented which are metallic scaffolds implanted at the site of the block to prevent re-block. In the last three decades, stents quality has significantly improved with fewer complications and excellent outcomes.
Although angioplasty was discovered way back in the 1970s, still till recently, complex cases were managed by bypass surgery. Examples of the complex cases are hard calcified blocks, tortuous vessels, multiple long blocks or blocks at difficult locations of the vessels etc. With cutting-edge techniques manging, these challenging scenarios have become possible via angioplasty. Internal imaging techniques like optical coherence tomography (OCT) or Intravascur ultrasound (IVUS) made it possible to properly delineate the properties of the blockades like the length of the block, presence of calcium or diameter of the stent to be used etc. So that a stent can be implanted in places like the left main coronary artery with ease. Guide extension catheters are become available for tortuous arteries where passing a balloon or stent is usually very difficult. Calcium cutting techniques like cutting balloons, rota ablation devices and the newest one in kitty intra vascular lithotripsy (IVL) have been introduced so previously unexpandable blocks now can be tackled. Some technical advances in angioplasty procedures themselves have been introduced like bifurcation stenting techniques have revolutionised the treatment of vessels with joints (bifurcating vessels). As mentioned previously, stents have become much more advanced and sophisticated so that long length blocks, small diameter vessels or very large vessels can be stented without fear of re-blockades.
So, with the advent of newer techniques, many complex blockades can be managed with coronary angioplasties now, however, the most important decisions are when to do the angioplasty when to manage medically or when to send the patient for bypass surgery which still has a major role in modern-day cardiology practice. This is decided by a ‘Heart team’ where cardiologists and cardiac surgeons discuss and decide about the best treatment option.
Mission — Healthy Hearts
Dr. Tamiruddin A. Danwade
Senior Consultant Interventional Cardiologis,
Mother and Rhythm Clinics,
Kharghar and Seawoods, Navi Mumbai.
+919321459928
मराठी अनुवाद
गुंतागुंतीच्या अँजिओप्लास्टी
आपले हृदय हे एक प्रचंड कार्यक्षमतेचे नैसर्गिक पंप आहे. ते संपूर्ण शरीराला रक्तपुरवठा करते. कोरोनरी धमन्या या तुलनेने लहान पण महत्वाच्या रक्तवाहिन्या असतात ज्या हृदयालाच रक्त पुरवतात. अनेक कारणांनी, मुख्यतः कोलेस्टेरॉल जमा झाल्यामुळे या रक्तवाहिन्यांमधे ब्लॉक तयार होतात त्यामुळे छोटा किंवा मोठा हृदयविकाराचा झटका येऊ शकतो जो जीवघेणा ठरू शकतो.
या ब्लॉक साठी पूर्वी बायपास शस्त्रक्रिया हा एकमेव उपचार पर्याय उपलब्ध होता. ही एक सुप्रा-मेजर शस्त्रक्रिया आहे ज्यामध्ये रिकव्हरी साठी जास्त वेळ लागतो, पेरीऑपरेटिव्ह काम्लीकेशन आणि मृत्युदर हेसुध्दा जास्त असतात. 1977 मध्ये, डॉ. आंद्रियाज आर. ग्रुंटझिग यांनी नवीन उपचार पध्दती शोधली – कोरोनरी अँजिओप्लास्टी. अँजिओप्लास्टी ही एक पर्क्यूटेनियस (नसांद्वारे करता येणारी)प्रक्रिया आहे ज्यामध्ये हृदयरोग तज्ञ कोरोनरी धमन्यांमधे तार त्यानंतर फुगा एका लहान नळीसारख्या कॅथेटरद्वारे पार करतात आणि त्याद्वारे रक्त प्रवाह सुधारण्यासाठी ब्लॉक काढले जातात. सुरुवातीला, ही एक साधी पद्धत होती, दुसरे काहीही केले जाऊ शकत नव्हते, नंतर, स्टेंटचा शोध लावला गेला ज्यामध्ये ब्लॉकच्या जागेवर री-ब्लॉक होऊ नये म्हणून मेटलिक स्कॅफोल्ड्स (स्टेंट) लावले जातात. गेल्या तीन दशकांमध्ये, कमी गुंतागुंत आणि उत्कृष्ट परिणामांसह स्टेंट्सच्या गुणवत्तेत लक्षणीय सुधारणा झाली आहे.
जरी 1970 च्या दशकात अँजिओप्लास्टीचा शोध लागला, तरीही अगदी अलीकडेपर्यंत, बायपास शस्त्रक्रियेद्वारे जटिल प्रकरणे ठीक केली जात होती. कठीण कॅल्सीफाईड ब्लॉक्स, वळनदार रक्तवाहिन्या, जास्त लांबीचे ब्लॉक्स किंवा वेसल्सच्या अवघड जागी ब्लॉक्स इत्यादी गुंतागुंतीच्या केसेसची उदाहरणे आहेत. अत्याधुनिक तंत्रज्ञानामुळे, ह्या आव्हानात्मक परिस्थितीत सुद्धा अँजिओप्लास्टीद्वारे उपचार करणे शक्य झाले आहे. ऑप्टिकल कोहेरेन्स टोमोग्राफी (ओसीटी) किंवा इंट्राव्हास्कूलर अल्ट्रासाऊंड (IVUS) सारख्या अंतर्गत इमेजिंग तंत्रांमुळे ब्लॉकेड्सचे गुणधर्म जसे की ब्लॉकची लांबी, कॅल्शियमची उपस्थिती किंवा स्टेंटचा व्यास इत्यादी योग्यरित्या रेखाटणे शक्य झाले आहे. आता स्टेंट डाव्या मुख्य कोरोनरी धमनी सारख्या अवघड ठिकाणी सहजपणे रोपण केले जाऊ शकते. गाईड एक्स्टेंशन कॅथेटर त्रासदायक वळणदार धमन्यांसाठी उपलब्ध आहेत जेथे फुगा किंवा स्टेंट पास करणे सहसा खूप कठीण असते. कॅल्शियम कटिंग तंत्र जसे की कटिंग फुगे, रोटा ऍब्लेशन उपकरणे आणि इंट्रा व्हॅस्कुलर लिथोट्रिप्सी (IVL) असे सर्वात नवीन तंत्रज्ञान आता उपलब्ध आहे जेणेकरुन पूर्वी अशक्य भासणारे ब्लॉक आता सहज हाताळले जाऊ शकतात. याशिवाय अँजिओप्लास्टी प्रक्रियेमध्ये सुद्धा तांत्रिक प्रगती केली गेली आहे जसे की द्विभाजन स्टेंटिंग (Bifurcation Angioplasty) तंत्राने जोड (दुभाजक वाहिन्या) असलेल्या रक्तवाहिन्यांच्या उपचारांमध्ये क्रांती केली आहे. आधी सांगितल्याप्रमाणे, स्टेंट अधिक प्रगत आणि अत्याधुनिक बनले आहेत जेणेकरून लांब लांबीचे ब्लॉक्स, लहान व्यासाच्या वाहिन्या किंवा खूप मोठ्या वाहिन्यांना पुन्हा ब्लॉकच्या भीतीशिवाय स्टेंट करता येते. जर ब्लॉक १०० % असेल आणि जुना असेल तर तो दगडासारखा कठीण होतो (CTO) हे हाताळण्यासाठी नवीन CTO तारा आता उपलब्ध आहेत ज्याने ही कठीण अँजिओप्लास्टी करणे शक्य झाले आहे.
नवीन तंत्रांच्या आगमनाने, आता कोरोनरी अँजिओप्लास्टीने अनेक जटिल ब्लॉक्सचा उपचार
केला जाऊ शकतो, तथापि, अजूनही काही ब्लॉक्समध्ये बायपास शस्त्रक्रिया हाच पर्याय असतो. अँजिओप्लास्टी केव्हा करावी किंवा रुग्णाला बायपास शस्त्रक्रियेसाठी केव्हा पाठवायचे हे सर्वात महत्त्वाचे निर्णय आहेत. हे ‘हार्ट टीम’ द्वारे ठरवले जाते जेथे हृदयरोगतज्ज्ञ आणि कार्डियाक सर्जन चर्चा करतात आणि सर्वोत्तम उपचार पर्यायांबद्दल निर्णय घेतात.
डॉ. तमिरुद्दीन अ. दानवाडे
हृदयरोगतज्ज्ञ, न्यूईरा हास्पिटल,
मदर & रिदम क्लिनिक,
खारघर आणि सीवूड्स,
नवी मुंबई.
फोन – +९१९३२१४५९९२८

Leave a comment